Job growth in the U.S. healthcare sector has been especially strong recently. Chart 1 shows that healthcare employment (blue bars) has grown by about 2.2 percent annually since 2011, with growth accelerating in the post-pandemic period to nearly 5 percent in 2024._ Within this overall expansion, care aides (patterned bars) have accounted for a growing share of both employment and job growth in the sector, with their share of healthcare employment (purple line) rising from about 11 percent in 2011 to nearly 17 percent in 2024._ Over this period, care aide jobs contributed nearly 40 percent of total growth in healthcare employment, suggesting that recent expansions in healthcare have been increasingly concentrated in labor-intensive care services.
Chart 1: Healthcare employment is growing, with care aides accounting for an increasing share of jobs
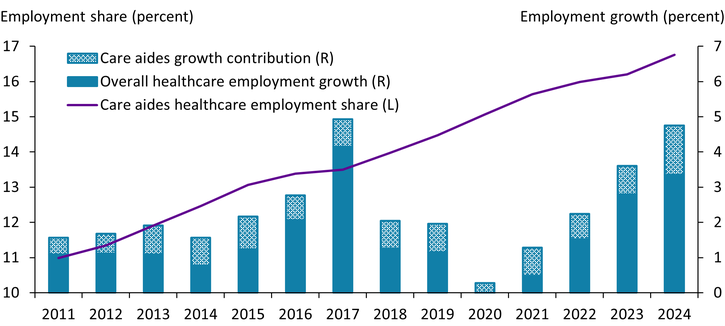
Notes: Care aides include home health and personal care aides. Employment series are adjusted for a break in occupational classification associated with the transition to the 2018 Standard Occupational Classification (SOC) codes to ensure comparability over time. The contribution to employment growth is defined relative to net healthcare employment growth and is shown cumulatively. 2020 healthcare employment growth is –2.4 percent and is omitted from the chart.
Source: U.S. Bureau of Labor Statistics.
An aging population appears to be an important driver of healthcare employment growth. Chart 2 shows that states with larger increases in their share of population age 75 and older also experienced larger increases in healthcare employment as a share of total employment._ This pattern is consistent with research showing that aging populations increase demand for health and long-term care services, suggesting recent healthcare employment growth represents a structural transformation of the labor market in response to an aging population._
Chart 2: States that experienced larger growth in their share of population age 75 and older tended to have larger growth in their healthcare employment share
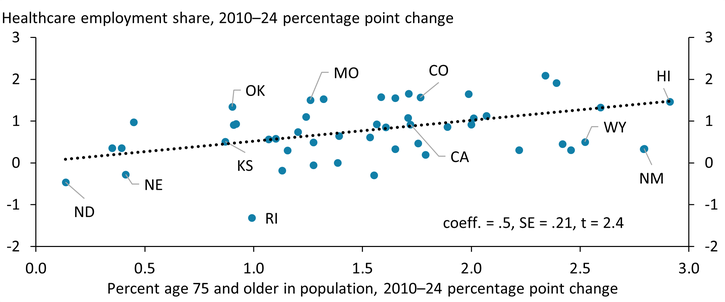
Notes: Data are from the American Community Survey. Healthcare employment is defined using industry codes. Outliers (Vermont and South Dakota) are excluded from the chart.
Source: U.S. Census Bureau.
Thus far, the healthcare sector has relied on a narrow segment of workers to support this growth. Chart 3 shows that healthcare workers (purple bars) are disproportionately female, with women accounting for 76 percent of healthcare employment. Care occupations (green bars) rely on an even more specific set of workers: 84 percent of care aides are women, 60 percent of care aides have a high school degree or less, and 30 percent of care aides are immigrants._
Chart 3: Care occupations disproportionately rely on female, lower-skilled, and immigrant workers
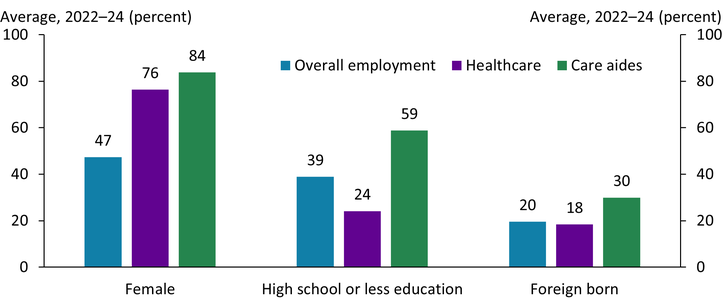
Notes: Data are from the American Community Survey. Care aides include home health and personal care aides.
Source: U.S. Census Bureau.
Two groups of workers that have been important sources of the healthcare labor supply may be approaching limits to growth. The left side of Chart 4 shows that labor force participation among prime-age (25–54) women recently reached an all-time high of 78.5 percent._ This increase has been supported in part by rising healthcare employment demand, given the sector’s heavy reliance on female workers. The right side of Chart 4 shows that at the same time, the foreign-born share of care aides has risen substantially, from around 24 percent in 2012 to around 31 percent in 2024. However, with current U.S. restrictions on immigration, immigrant flows are expected to remain low in the coming years, constraining a key source of care workers._
Chart 4: Prime-age female labor force participation reaches all-time high while immigrant share of care aides rises
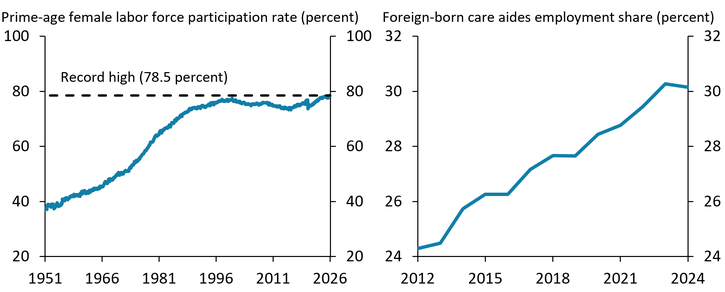
Notes: The foreign-born share of care aides is calculated using data from the American Community Survey. Care aides include home health and personal care aides.
Sources: U.S. Bureau of Labor Statistics and U.S. Census Bureau.
Together, trends in women’s labor force participation and the share of immigrant care aides raise questions about the sustainability of the healthcare sector’s labor supply, especially in the face of growing demand. How much female labor force participation can continue to increase from its current all-time high is unclear, and aging could either increase the need for informal care within families—pulling women out of the labor force—or expand demand for formal care in the healthcare sector—drawing women into the labor force. Additionally, the supply of immigrant labor is expected to contract even as demand for caregiving occupations increases. Thus, if labor supply cannot keep up with demand, caregiving costs could rise, potentially shifting more care back to households and reducing female labor supply._
Overall, an aging U.S. population is driving rapid growth in healthcare employment, particularly in care-intensive occupations. So far, this demand has been met largely by women and immigrant workers. However, with female labor force participation at historical highs and immigration flows expected to remain constrained, the healthcare labor supply may face challenges to further expansion.
Endnotes
-
1 Care aides refer to occupations under Standard Occupational Classification (SOC) code 31-1120 (Home Health and Personal Care Aides). Home Health Aides (31-1121) provide routine individualized healthcare such as changing bandages, dressing wounds, and administering medication to patients in their homes or residential care facilities. Personal Care Aides (31-1122) assist with activities of daily living, such as bathing, dressing, grooming, meal preparation, and companionship for elderly or disabled individuals. Both occupations require high levels of direct physical interaction and are difficult to substitute with capital or technology.
-
2 The 2017 increase should be interpreted with caution, as a significant component of it likely reflects a break in Occupational Employment and Wage Statistics (OEWS) measurement associated with changes in definitions and reporting for healthcare occupations.
-
3 Using overall healthcare employment rather than only care aides helps capture the broader labor market response to aging, as rising care needs increase demand not only for aides but also for other healthcare and support occupations.
-
4 Grabowski, Gruber, and McGarry (forthcoming) show that aging reshapes labor demand and increases use of health and long-term care services.
-
5 Chidambaram and Pillai (2025) show that immigrants make up a large and growing share of the direct long-term care workforce, especially in home care settings.
-
6 Bauer and Wang (2023) show that prime-age women’s labor force participation exceeded its prior all-time high beginning in February 2023.
-
7 Grabowski, Gruber, and McGarry (forthcoming) find that increasing immigration significantly raises staffing levels in U.S. nursing homes, especially in full-time positions.
-
8 Maestas, Messel, and Truskinovsky (2024) report that women’s employment falls by about 2.7 percentage points in the three years after caregiving begins, with earnings also declining.
Article Citation
Cohen, Elior. 2026. “Can Healthcare Labor Supply Keep Up with Aging-Driven Demand?” Federal Reserve Bank of Kansas City, Economic Bulletin, May 1.
References
Bauer, Lauren, and Sarah Yu Wang. 2023. “External LinkPrime-Age Women Are Going Above and Beyond in the Labor Market Recovery.” Brookings Institution, August 30.
Chidambaram, Priya, and Drishti Pillai. 2025. “External LinkWhat Role Do Immigrants Play in the Direct Long-Term Care Workforce?” KFF, April 2.
Grabowski, David C., Jonathan Gruber, and Brian E. McGarry. Forthcoming. “External LinkImmigration, the Long-Term Care Workforce, and Elder Outcomes in the U.S.” American Journal of Health Economics.
Maestas, Nicole, Matt Messel, and Yulya Truskinovsky. 2024. “External LinkCaregiving and Labor Supply: New Evidence from Administrative Data.” Journal of Labor Economics, vol. 42, no. S1, pp. 183–218.
Elior Cohen is a senior economist at the Federal Reserve Bank of Kansas City. The views expressed are those of the author and do not necessarily reflect the positions of the Federal Reserve Bank of Kansas City or the Federal Reserve System.
Author
